-If
the embryo is seen , measure crown-rump length , if this is greater than 6 mm
with no evidence of fetal heart pulsation , appearance is highly suggestive of
missed miscarriage , then you should inform patient and repeat exam after 7
days as discussed before.
D.D. of a gestational sac with no fetal
node and no fetal heart pulsation (this could be )
Points to remember:
-A
mean sac diameter more than 20 mm with no evidence of fetal pole or yolk sac is
highly suggestive of anembryonic
miscariage.
-A
CRL greater than 6mm with no evidence of a fetal heart pulsation is highly
suggestive of missed
miscarriage.
-A
repeat trans-vaginal scan after 7 days later should confirm diagnosis.
 |
| Anembryonic miscarriage with evidence of
a collapsed sac with diameter more than 20 mm and no evidence of fetal pole or
yolk sac. |
 |
| Missed abortion characterized by presence
of a fetal pole inside a fetal sac but without fetal heart pulsation |
This 1st trimester patient complained of
pain in the lower abdomen. Sonography of the gravid uterus shows an anechoic
collection (blood--> see arrows) in the upper part of the gestation sac
between the decidual tissue and the chorion. There is also evidence of
separation of the margins of the early placenta (abruption). The embryo, in
this case, showed cardiac activity. These ultrasound images are diagnostic of
sub chorionic hematoma. It is advisable to follow this case with repeat
Sonography after 1 week and closely monitor the hematoma.

This 1st trimester patient complained of
pain in the lower abdomen. Sonography of the gravid uterus shows an anechoic
collection (blood--> see arrows) in the upper part of the gestation sac
between the decidual tissue and the chorion. There is also evidence of
separation of the margins of the early placenta (abruption). The embryo, in
this case, showed cardiac activity. These ultrasound images are diagnostic of
sub chorionic hematoma. It is advisable to follow this case with repeat
Sonography after 1 week and closely monitor the hematoma.
Trans-vaginal sonogram . The absence of
the gestational sac and the presence of intrauterine debris are typical of a
incomplete abortion with retained
products.
Abortion in progress in a patient with a
history of vaginal bleeding. Transvaginal US image of the uterus demonstrates a
low-lying gestational sac (arrow) with mixed hyper- and hypo echoic contents in
the endometrial cavity of the fundus (arrowheads), which represent decidual
reaction and hemorrhage. The patient experienced a complete spontaneous
abortion a few hours after the US examination.

 This 1st trimester patient complained of pain in the lower abdomen. Sonography of the gravid uterus shows an anechoic collection (blood--> see arrows) in the upper part of the gestation sac between the decidual tissue and the chorion. There is also evidence of separation of the margins of the early placenta (abruption). The embryo, in this case, showed cardiac activity. These ultrasound images are diagnostic of sub chorionic hematoma. It is advisable to follow this case with repeat Sonography after 1 week and closely monitor the hematoma.
This 1st trimester patient complained of pain in the lower abdomen. Sonography of the gravid uterus shows an anechoic collection (blood--> see arrows) in the upper part of the gestation sac between the decidual tissue and the chorion. There is also evidence of separation of the margins of the early placenta (abruption). The embryo, in this case, showed cardiac activity. These ultrasound images are diagnostic of sub chorionic hematoma. It is advisable to follow this case with repeat Sonography after 1 week and closely monitor the hematoma.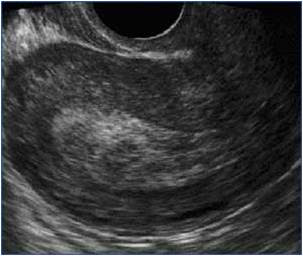 Trans-vaginal sonogram . The absence of the gestational sac and the presence of intrauterine debris are typical of a incomplete abortion with retained products.
Trans-vaginal sonogram . The absence of the gestational sac and the presence of intrauterine debris are typical of a incomplete abortion with retained products. Abortion in progress in a patient with a history of vaginal bleeding. Transvaginal US image of the uterus demonstrates a low-lying gestational sac (arrow) with mixed hyper- and hypo echoic contents in the endometrial cavity of the fundus (arrowheads), which represent decidual reaction and hemorrhage. The patient experienced a complete spontaneous abortion a few hours after the US examination.
Abortion in progress in a patient with a history of vaginal bleeding. Transvaginal US image of the uterus demonstrates a low-lying gestational sac (arrow) with mixed hyper- and hypo echoic contents in the endometrial cavity of the fundus (arrowheads), which represent decidual reaction and hemorrhage. The patient experienced a complete spontaneous abortion a few hours after the US examination.






No comments:
Post a Comment